Early in his career, Dr. Humphreys admitted, “How dare these people do things that I have all these degrees to do?”
Many of us associate Alcoholics Anonymous (AA) with collective Bible-thumping. To be in AA is to become a sobriety Evangelist who walks with the Lord toward abstinence, reminding everyone of their journey as frequently as possible. This soft evangelism can overpower the benefits of group participation.
Now that we’ve throat-cleared the negative aspects of cult-like collusion, we turn to the undeniable positives of such fellowship. On a broad scale, group affiliation helps to forge a sense of identity. This is where comparison and even some constructive shame play a pivotal role in shaping how we behave and what we believe to be true. We require connection with others to not only understand ourselves and our values, but to more thoughtfully (and honestly) assess our abilities. Although comparison has been demonized, it’s critical in determining how our own behavior will come about. An honest sense of self is impossible to develop without the influence of “the other”; how else would we know if we broke a state record? Are we truly exceptional at a skill if we’re not cross-referencing our scores with that of those better? How would we know if we scored in the top percentile on the board exam? Or if we’re superior critical thinkers, or if we’re larger-hearted than our co-workers? While leaning too much into the opinions of others, they are critical in who we are and what we believe to be true.
Thanks for reading honestly unorthodox.! Subscribe for free to receive new posts and support my work.
Social contagion is a strong force, and our drive to belong is what makes organizations like AA so useful in drawing out adaptive behavior. To maintain relationships with like-minded others is to engage in similar habits. If our group is health-minded, for example, and we wish to preserve these ties, we must also become health-minded.
In our pursuit of individual wellness, which can sometimes come at the expense of other people (e.g., “Be selfish and only focus on you and your needs!”), it’s imperative we see health behavior as a group effort. Of course there are intrapersonal problems that influence our decisions. Individual motivations, an inability to tolerate criticism, ruminating over negative events of the day, family history of illness, genetics--- all of these factors converge to play a role in our habits. But even amidst our internal problems, we function only as a miniscule portion of a colossal, ever-changing, eclectic culture. And our environment plays a larger role than we think. Look at our mental health crisis (which I don’t think is a crisis, as I stated in Part One): in the past 4-5 years, internal problems, like nervousness, “burnout”, “imposter syndrome”, anxiety, and depression, became a collective panic. In turn, we rallied together to mediate the symptoms we thought needed fixing (even if these efforts were distorted, ridiculous, and ass-backwards). Trigger warnings, DEI initiatives, texting-therapy, social-emotional learning, and mental health days--- these were widespread, organizational-level shifts in behavior, shifts that still largely remain in place. Even our nation’s most prestigious universities offered safe rooms and hot chocolate to students in a state of delusional alarm. Affiliation goals (read: social contagion), whether adaptive or criminally loony, are largely ignored in the movement toward wellness. Let’s fix that.
TO RUMINATE IS TO BOND
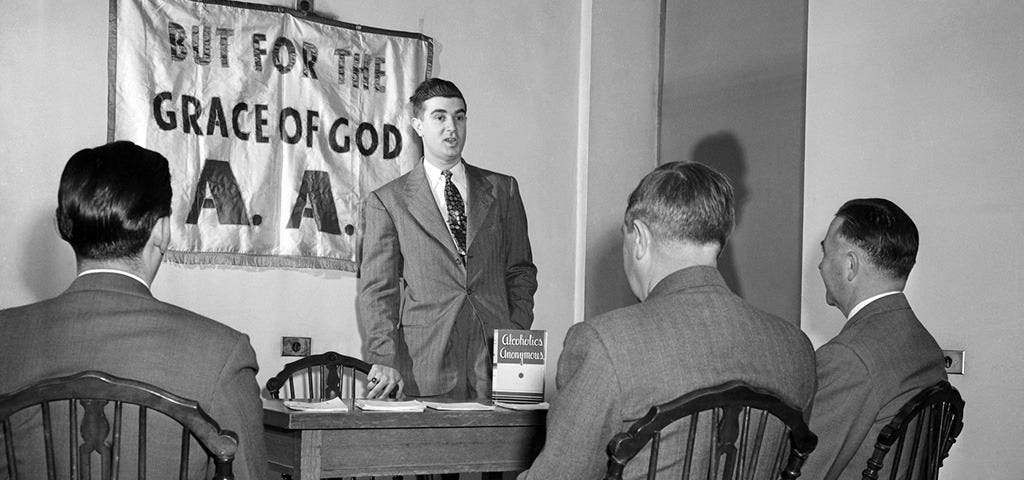
Alas, we return to the covenant that is alcoholic bonding. AA is the most well-studied “intervention” as it relates to helping alcoholics, with AA being more effective than psychotherapy in nearly 100% of studies. This is profound, as AA is not a clinical or even therapeutic method, requiring zero licensure to operate and provide services. In the grand scheme of our culture, which medicalizes everyday problems and offers up only billable providers as gold-standard treatments, it’s perhaps deflating to the people who have spent hundreds of thousands of dollars to be licensed only to find a junkie is more convincing in getting people on the wagon. Keith Humphreys, a psychiatrist and professor of psychiatry and behavioral science, evaluated 35 studies of AA’s efficacy with over 10,000 participants. What he found? Continued participation in AA was not only the most effective in achieving abstinence, but a powerful force in lowering healthcare costs for each member. What other initiative has been successful in lowering healthcare cost? Robert F. Kennedy (RFK), a long-time advocate of AA for his own addiction, is aware of this potential for societal change.
RFK and proponents of the MAHA movement have exposed obscene healthcare costs from our largest and most trusted medical establishments in recent weeks, and I imagine they’re itching to offer alternative solutions to the nation’s constellation of illness. I’m admittedly swell with glee that they haven’t suggested a need for more therapeutic services.
I spoke in parts one through four about the God complexes surrounding healthcare, specifically mental and behavioral healthcare. I can understand why licensed professionals are skeptical about organizations like AA, who are run by everyday people who operate not on clinical or professional philosophies but on anecdotal experience alone. Fields like mine (behavior analysis), stand appalled at most any success story which does not come replete with data or documentation. I can understand this, to a degree. With emotions being unreliable indicators of reality, we must rely on objective information to make sound decisions. But you don’t need to hire a licensed professional to learn to do this.
Early in his career, Dr. Humphreys admitted, “How dare these people do things that I have all these degrees to do?”
I would be remiss if I didn’t emphasize the following: AA will not work for everyone. Even staunch advocates of AA will remind you that their principles, although sacred to them, may not be what certain people need. The same can be said about any single intervention, whether that be educational, medicinal, or therapeutic. This fact, paired with our culture’s insistence on hyper-individualism, seems at least part of the reason why our healthcare system has split into so many specialized silos. Doing so provides the illusion that our problems are special, and that basic strategies like healthy lifestyle habits and community connection couldn’t possibly address such complexity.
A KINK FOR BEHAVIORAL MIMICRY
We must understand and embrace the social theory of behavioral mimicry to see our culture move toward health. Behavioral mimicry, as in, we copy people when we wish to be around them and maintain friendships. A crackhead and a Hyrox competitor, for example, will struggle to preserve any form of a bond. Their lifestyles and values are far too different. The Hyrox athlete who leads a healthy lifestyle will gravitate towards others with similar value systems and habits, while the crackhead will do the same in his own scrappy neck of the hood. Interestingly, though, we’re more inclined to copy the behavior of another person if they exude warmth and engage us in interaction. It’s not enough, then, to be a digital health influencer who wears leggings that resemble assless chaps and remind people to lean into their values. Being “the girl next door” or even “educating” people on the benefits of eating more protein and doing more cardio is unsurprisingly unsuccessful should more global impact be the goal. Transactional and cold exchanges, even if unintentional, are less likely to sway the behavior of another person. Scare tactics, like DARE and other nation-wide school prevention programs, are equally futile. In short, a person is more likely to adopt behavior (whether positive or negative) if it means it’ll protect their social ties and their identity.
In understanding our thirst for belonging, would it be useful to offer more group-and-community-oriented services for those struggling? As opposed to the unsustainable, draining, often times unnecessary one-to-one work of a psychotherapist and a patient, ruminating over problems? Dr. Peter Gray, who speaks frequently about the wellness-and-parenting-culture resulting in narcissism in children, found scathing reviews of individualized-mental-health-therapy for children. In one study out of Australia, teens who attended an 8-week “workshop” on mental health reported poorer quality of life, significantly more depression and anxiety, and poorer relationships with their parents, who were also part of the workshop. In another study, a program involving mindfulness training for children ages 11-13 resulted in poorer social and emotional functioning. Perhaps all of this singular, internal rumination does not actually “normalize emotions” and “better socialize” children. Is the individualized nature, then, the problem? After all, how feasible is it to account for every single person’s emotional experience?
UBUNTU FOR THE FUTURE
Collectivist cultures like those in Africa abide by a standard called “Ubuntu”, which is not present in Western cultures, as it refers to a communal system in which everyone is bound as one, despite being separate beings. According to this value system, “the self is perceived in relation to the group… the problems and demands of one person are the problems and demands of everyone.” Perhaps the modern wisdom that is, “that sounds like a you problem” is reaching its rightful retirement.
While I’m not making the argument that every stressor be handled communally, there are aspects of collective value systems that would benefit people in distress. We cannot argue the facts that public figures like Dr. Vivek Murthy, our Surgeon General, have made regarding loneliness. He has escalated an experience of disconnection to that of a public health emergency, with the negative physical effects of social disconnectedness being comparable to smoking and sedentarism. Adults rate their relationships as the most important facet of their lives and as the most abundant sources of meaning and purpose. To guide people towards entanglement in their own problems (i.e., sitting and ruminating over problems alone or with a single therapist) seems entirely counterintuitive when we understand the broader impact of social connectedness on our behavioral, physical, and mental wellbeing. We mentioned earlier ways in which social contagion naturally occurs, for better or for worse, when social dyads begin to form. We must leverage our natural tendency toward kinship should we hope to change wellbeing on a nation-wide scale.
I understand that grouping people together comes with its own flaws. If a skilled lead is not assigned, the session can quickly devolve into a semantic pissing contest. It can also encourage spiraling, problem-focused behavior should a lead fail to direct complaints and grievances toward solution-oriented decisions. But can’t the same be said about any situation we’re in outside of our home? I remain unconvinced that the costs outweigh the immense benefits of group affiliation, particularly in regards to managing our nation’s approach toward physical and mental health. The old adage, “it takes a village” could not ring more true.
Perhaps we revolutionize the referral process in mental and behavioral health clinics to one which requires an individual to show proof of commitment to the basic facets of wellbeing. As can be seen in the above visuals, our wellbeing is comprised of separate parts which all assemble to form a person functioning at their “optimal”. I’d wonder how simply recruiting accountability partners, instead of licensed professionals, would lessen the unnecessary demand on psychological professionals. I’d wonder how psychiatrists prescribing exercise, balanced diets, and social connection would change the mass psychotropic assault on our serotonin receptors. And I’d wonder how this “mental health crisis” would collapse should we give it the middle finger by banding together as we have throughout every single disaster in human history. Holocaust survivors pride themselves on not only their strength in the face of unfathomable adversity and hatred, but their ability to hold positive regard in their future interactions. You will not speak to a Holocaust survivor who harbors contempt, or recommends that your sense of “you” demands a specific chemical balance only achievable through professional service.
Viktor Frankl reminds us that “those who have a ‘why’ to live, can bear almost any how.” We have our sense of why. Let’s help others find theirs. And I’m confident we’re equipped to handle all of life’s “hows”.
Thanks for reading honestly unorthodox.! Subscribe for free to receive new posts and support my work.