Note: If you haven’t, please read Jeanne Lenzer’s recent piece, “The Campaign to Turn Healthy People into Alzheimer’s Patients.” Jeanne is a brilliant and ferocious journalist, and her piece prompted me to dig into the research history behind it. The next few weeks will be like the Cholesterol Mistake Series: short pieces describing precisely how Alzheimer’s research has been misinterpreted and distorted. The Alzheimer’s Mistake Series is my attempt to explain how we got here.
“Is it some weird poison??”
Nicole, our PA, held up a catheter bag. The urine in it was purple—bright purple.
“I drew bloods, started a line, and paged renal. Antibiotics?” She added, grimacing, “This can’t be good.”
I looked first at the chart, then at the man, who sat comfortably, sipping ginger ale and giggling at The Price is Right.
“No need,” I said. “And you can cancel the consult.”
RT is entirely reader-supported. I’d like to keep doing it, so please become a paid subscriber.
Purple Urinary Bag Syndrome, as it’s known, is a thing—and it is something to behold. The enzymes and bacteria in urine can, on rare occasion, blend to form a witch’s brew that looks like grape soda. But the color, which lasts hours to days, is typically the only ‘problem’ in PUBS. The condition is all bark, and no bite.
Which means there’s no reason to risk antibiotic resistance and side effects, or a monster hospital bill for a monster work-up. In essence, PUBS is little more than a master class in visual distraction.
Purple urinary bag syndrome
Unfortunately, that is a pitfall that has historically sent modern medicine into convulsions of self-defeat. Today, for instance, we are living with the fallout from a distraction first glimpsed in 1906 by a German researcher named Alois Alzheimer.
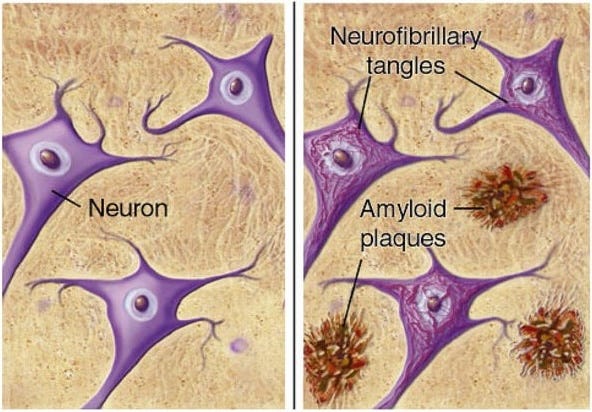
Dr. Alzheimer first identified the amyloid plaque, a nasty looking clump of waste found in the brain of a woman who had died of severe, early-onset dementia. That plaque spawned a neurology obsession. Later named Alzheimer’s Disease, the condition is a syndrome of clinical dementia with memory loss that was eventuallydefined partly by the detection and measurement of those clumps, which are often present on autopsy.
Amyloid plaques
But they’re not always present. Autopsy data show that amyloid plaques are an inconsistent presence in Alzheimer’s—nowhere near the kind of reliable presence that might suggest amyloid as the main cause of Alzheimer’s.
Yet sadly, much like cholesterol and the Lipid Hypothesis, in the 1990s dementia researchers bypassed the most fundamental rule of epidemiology: Before you crown a risk factor the main cause, you must prove it IS a risk factor.
The rule is unforgiving. If a single factor causes a disease, it should mathematically and reliably predict the disease. With smoking and lung cancer, that association is ironclad. With blood pressure and strokes, it does not falter.
But with Alzheimer’s Disease and its supposed culprit—beta-amyloid protein—the association failed from the beginning. (Sound familiar?). Two seminal papers, one by Terry in 1991 and a second by Arriagada in 1992, are among the most cited studies in the history of the field. Both are autopsy studies, and both found zero statistical relationship between amyloid plaque burden and clinical dementia.
Title page and a scatterplot from Arriagada et al, 1992, showing no association (‘NS’ = nonsignificant) between amyloid plaque—the target of current Alzheimer’s drugs—and Alzheimer’s Disease
In late 1991 Terry et al. found memory loss had no connection to amyloid plaques, and a year later Arriagada’s scatterplots (above) confirmed the same finding visually.
Despite these landmark reports being fundamentally inconsistent with amyloid plaques as a cause of Alzheimer’s, the neurology research community swept them aside and plowed forward with the Amyloid Hypothesis. Why? Perhaps, in part, because under a microscope the plaques look like wreckage—they are visually striking.
But they are a distraction.
In neurology this discrepancy is called the ‘clinico-pathologic disconnect’ and in the research community it is widely known: The brains of many who die with Alzheimer’s have little or no plaque, and most who die with plaque have little or no Alzheimer’s. In fact, autopsies show that the brains of cognitively normal elderly people are often riddled with amyloid plaques.
And yet, even as this disconnect became obvious, the die had already been cast. Starting in the late 1980s billions of research dollars and pharmaceutical budgets were being chained to the Amyloid Hypothesis, the unassailable premise that amyloid plaques cause Alzheimer’s Disease. This bizarre conclusion, unsupported by the most basic standards of evidence, spawned careers, research centers, and massive clinical trials, all laser focused on preventing and removing amyloid plaques.
Therefore, predictably, when the research from these endeavors began rolling in, the amyloid chickens came home to roost.
Next week, in Part 2, I’ll show you how demented mice and the trial of a highly toxic vaccine led unscrupulous researchers to invent a savior for their failed Hypothesis.
And how it became one of the most famous, and disastrous, scientific frauds of the century.