Author note: What follows is part 2 of a series intended to summarize and explain just how, historically, we went off the rails with cholesterol. Check out part 1 here.
In the early 1990s, Eugene Braunwald and the cardiology community had a problem.
In the throes of a major heart attack new clot-buster drugs and angioplasty procedures were working—saving lives. Cardiologists could see it even months later, in the clinic.
But they couldn’t see it in the data.
Published trials were short, lasting weeks or months. But reperfusion—re-opening occluded arteries with drugs or procedures—didn’t just prevent instant deaths. It also halted and reversed massive heart attacks, rescuing enough heart muscle to prevent heart failure and deaths that result months or even years later. The benefit was real, but delayed. And therefore invisible in trials.
Braunwald and his colleagues therefore fashioned a solution.
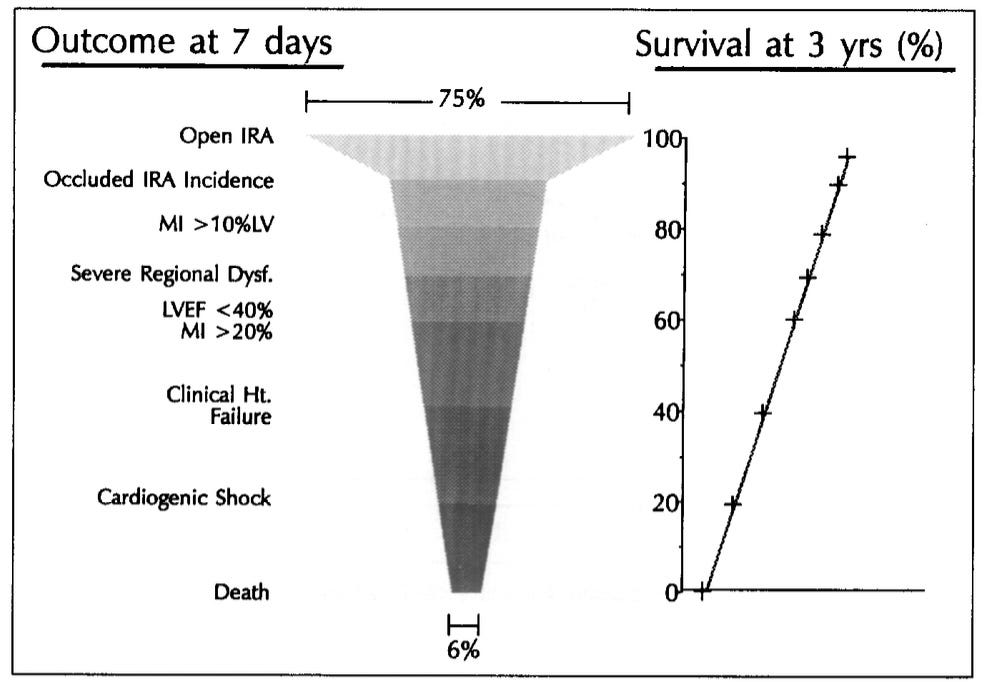
They noted: Not all myocardial infarctions, i.e. heart attacks, are equal. While small MIs often pass without danger, big ones that damage lots of heart muscle can cripple a heart, leading to failure, decline, and death. In these cases even supposedly ‘nonfatal’ ones are a harbinger—a surrogate—for delayed disability and death.
In a landmark paper they called on researchers to therefore count not just deaths, but also these large ‘nonfatal MIs’.
The paper mapped risk carefully, detailing a hierarchy: Larger infarcts predicted death, while small ones rarely did.
The argument was elegant, mathematical, and tightly anchored to both context (heart attacks in progress) and definition (big ones). And it worked. Reperfusion was shown to be a game-changer.
Then, ‘nonfatal MI’ was hijacked.
Braunwald’s careful creation was relocated and redefined. Transposed into trials of prevention (rather than heart attacks) and expanded to include any attack (not just big ones), ‘nonfatal MI’ became something entirely different.
In prevention studies of healthy people nonfatal heart attacks are infrequent. They’re also heterogeneous, and—crucially—not dangerous. Why? Because the trials run for years. Big, dangerous heart attacks that lead to medium-term heart failure and death are easily captured.
In this context ‘nonfatal MI’ therefore no longer means large heart attacks with important and often fatal effects, it means overwhelmingly small ones, where even medium-term death is a virtual impossibility. Unlike nonfatal strokes, which sometimes leave people permanently disabled and dependent, small heart attacks do not.
Thus ‘nonfatal MI’, a term that for Braunwald meant a harbinger of death, became the opposite: a mark of guaranteed survival.
And we knew this early.
Fibrate drug trials of lowering cholesterol in the 1980s found that despite preventing nonfatal MIs, more people taking the drugs died. This debunked ‘nonfatal MI’ as a surrogate for death in prevention trials. Citing the frightening incongruity, a BMJ meta-analysis called for a moratorium on all cholesterol-lowering drugs.
And yet, nonfatal MI did not disappear—it grew. Soon it was the backbone of all cholesterol lowering trials, and the darling of industry researchers.
Why? Because rather than indicating mortal risk, nonfatal MI now distracted from it, functioning as a decoy that pulled the reader’s eye from outcomes people care about: disability, heart failure, dependence, death.
Take WOSCOPS, the trial that first ‘proved’ lowering cholesterol in primary prevention was worthy. In WOSCOPS there was no reduction in death. Or deaths from heart disease. Or strokes.
The only difference between groups was in ‘nonfatal MI’.
Across decades of trials that are now embedded in guidelines, the touted benefits are simply never driven by death, disability, heart failure, or stroke. They are driven by a proxy for guaranteed survival.
Remove ‘nonfatal MI’ from the measurement, and any advantage disappears.
Today the bait-and-switch is even more extreme than in WOSCOPS. Troponin blood tests are a newer gold standard for diagnosing heart attacks, precisely because they capture increasingly smaller—ultimately microscopic—events. These are now labeled heart attacks, but would literally never have registered in earlier trials. Braunwald would have called them ‘angina’, a far cry from the massive, disabling events he fought to include as an endpoint in trials.
Recognizing that nonfatal MI was failing as a surrogate for mortality, in 2021 researchers studied it. Analyzing decades of data in 144 studies, they found zero connection between nonfatal MI and death—the outcome it is supposed to herald.
Below are the key scatter plots from the paper, preceded by an example of what they should look like if nonfatal MI is a surrogate—as Braunwald intended. While none of the graphs even hints at a meaningful association, note Figure ‘2C’, where the analysis includes studies focused on the association between nonfatal MI and death over time.
That is not a surrogate. It is a decoy.
Would we all like to avoid even tiny heart attacks? Of course. But by center-staging events that are often microscopic, and basically preclude serious consequences, we risk medicalizing the equivalent of cardiac wrinkles.
Skin ages. It wrinkles, thins, and loses elasticity. So do coronary vessels. They stiffen, crack, and change. But if these changes never affect life span or function, should they be treated as equal in studies to a paralyzing stroke? Or crippling heart failure? Or death?
Right now, they are.
Which has led generations of well-intended doctors to conflate the findings reported in cholesterol trials with life-altering or life-saving effects.
Which, by definition, they are not.
And that is the fatal mistake of nonfatal MI—the engine that manufactures cholesterol-lowering ‘benefit’.
Next week, in part 3, we’ll look at cholesterol-lowering trial results through the prism of part 1 (LDL as a non-risk factor) and part 2 (nonfatal MI as the driver of benefit).