During the Cholesterol Mistake series, we’ve walked through the unraveling of a medical dogma.
First, we saw how the Lipid Hypothesis violates the seminal rule of risk factors. Next, we watched the goalposts shift from extending life to chasing non-fatal laboratory endpoints. Then, in trial appendices, we found the Big Mistake: tallying checkbox diagnoses while ignoring what matters to people.
Along the way, with new eyes we saw the subterfuge in a breaking cholesterol trial that failed to help humans, yet claimed victory. Then we unwound the stilted logic and murky math that allows a guideline to quietly serve itself.
Finally, we discussed ideologic gumption, the driver of a religious faith—cholesterolism—that eschews reason, logic, and scientific method.
How do we stop the momentum? How do we right-size cholesterol culture and help 25 million healthy people avoid a lifetime of pills that, if informed, most would not choose?
The answer lies in a simple truth: There is more power at your end of the stethoscope than you have ever been led to believe.
For decades, the clinic dynamic has been asymmetrical. The doctor holds the clipboard, interprets the guidelines, and hands down a prescription. But reform doesn’t start with new guidelines from the AHA. It starts with information symmetry (the goal of this Substack).
The solution to the Cholesterol Mistake—and nearly every other systemic problem in modern medicine—is to stop asking for the prescription and start asking for the information.
Here, then, is a playbook for your next appointment.
When your doctor suggests taking—or staying on—a statin, do not accept or refuse. Instead, ask for the math. Right there in the exam room ask your doctor to pull up the guideline’s new calculator. Together, calculate your 10-year risk for ASCVD.
With the result in hand insist on absolute truth, not relative. If the drug offers a ‘30% relative reduction’ and your baseline risk is 5%, together you can calculate your absolute reduction as 1.5% over ten years.
With that 1.5%—a 1 in 67 chance of benefit—hanging in the air, ask the critical follow-up: “What is my chance of getting diabetes or muscle damage from the drug during that same decade?”
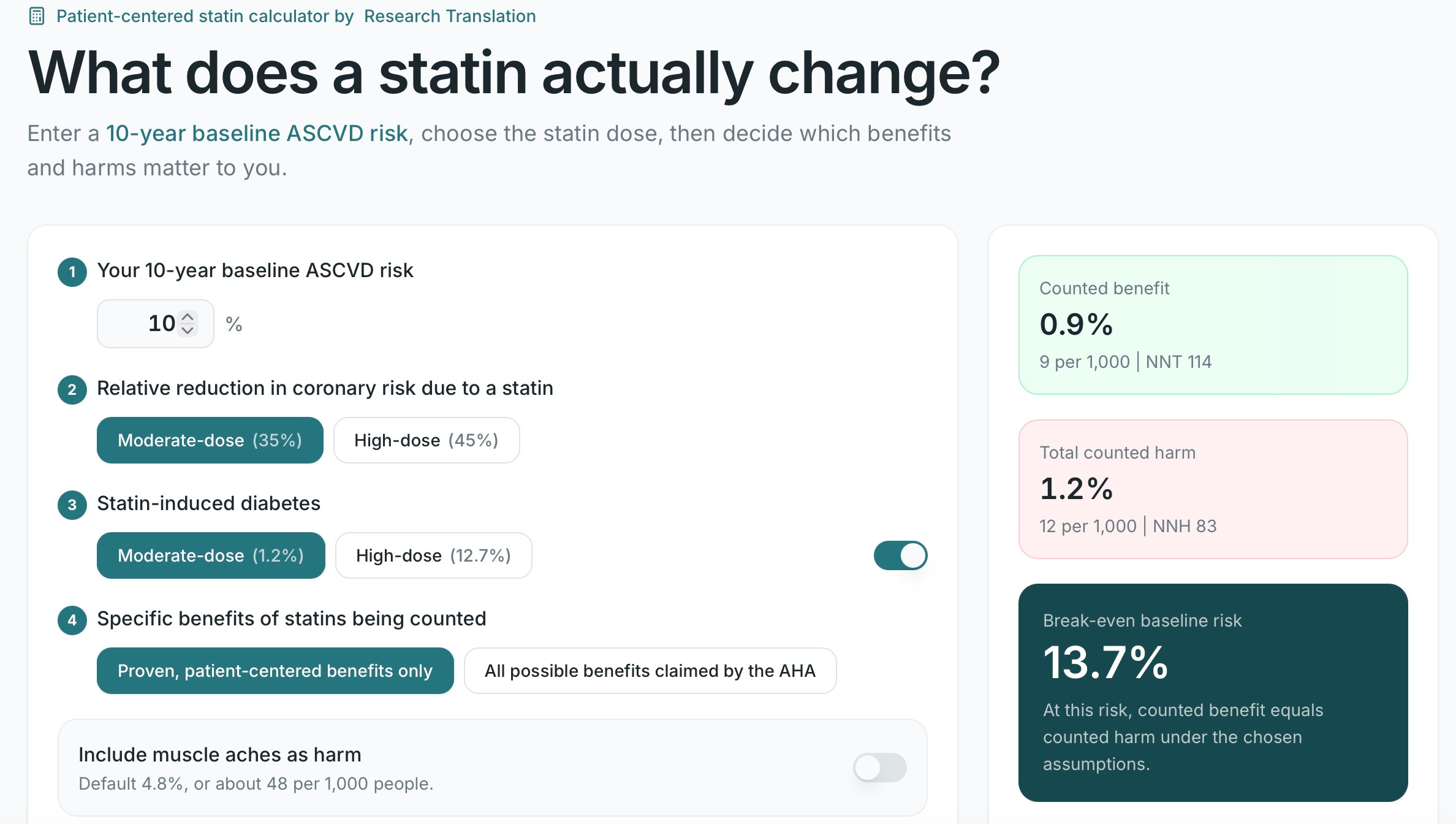
To make the numbers transparent, use the Research Translation calculator—crafted just for statins, and just for this conversation:
Doctors overwhelmingly have good intentions, but they’re trapped in an experiential delusion, conditioned to treat the guideline rather than the person. By forcing them to articulate the absolute benefits alongside harms, you can break the spell.
Any physician unable to explain the data behind the pill will suddenly have to figure out how.
Evidence-based medicine isn’t just for doctors. The data belongs to you. By insisting on seeing the science, you restore the balance of power.
The era of blindly swallowing the Lipid Hypothesis is over. It is time to do the math—and show it.