The AHA’s new cholesterol guideline is asking professionals to start earlier, screen more, and treat cholesterol more aggressively, decades before any heart or vascular disease could plausibly occur. What follows, therefore, is the first of a series in which I will attempt to show how doctors (and most others) have misunderstood the science on cholesterol, from the beginning. I will be citing and showing original data from seminal studies, to help clarify what went wrong in translation, and how we can use the same data, productively, today.
----------
“Right there,” the man winced as I pressed on McBurney’s point. It hurt him to palpate his abdomen on the right side, two thirds of the way between his belly button and his pelvic bone.
I ordered a CAT scan and blood work, then presented the case to my attending. “Appendicitis” I said, with a flourish. “I called surgery, they’re on their way.”
Later, I found the attending scrutinizing the CAT scan results. He turned from the computer, and looked me in the eye. “This gentleman has no appendix. Had it out years ago. Other thoughts?”
In the early days of modern medicine, before guidelines and consensus statements, there was a simple rule:
**BEFORE YOU TREAT A RISK FACTOR, YOU MUST PROVE IT IS ONE**
That rule, a first principle in epidemiology, built everything. It built Framingham. It built the case for controlling blood pressure. It built the case against smoking. And it rests on a straightforward sequence:
First, find a characteristic like high blood pressure, or obesity, or smoking. Then look for strong, consistent associations with bad outcomes like heart attacks, strokes, and death.
These associations, however, cannot be tenuous. They must be mathematically robust and durable—across populations, and over long stretches of time.
If you find that ironclad association, then (and only then) you may ask whether changing the characteristic can prevent bad outcomes. But the association comes first.
Smoking is a risk factor that is robust and durable. It is associated, everywhere and always, with heart attacks, strokes, and death. High blood pressure is the same.
These relationships don’t flicker. They don’t disappear when you follow people longer. They don’t depend on how you slice the data.
But with cholesterol, they don't just flicker. They are almost entirely absent.
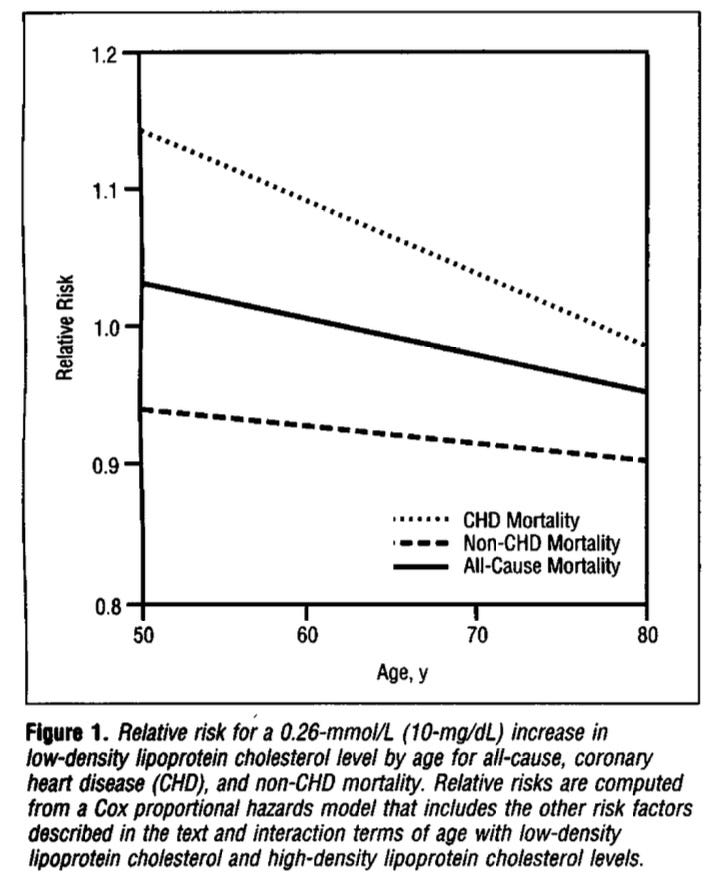
Fun fact: In the original Framingham study—the origin story for cardiovascular risk—LDL cholesterol was not a risk factor for death.
Below is a graph from the final paper. The solid line represents overall mortality. It crosses 1.0, and never strays far above or below. Mathematically, in other words, there is no relationship between mortality and LDL.
No important study has ever found the same for high blood pressure or smoking.
But it’s not just death. LDL, the ‘bad cholesterol’, has no relationship to any of the outcomes that matter most: Stroke? No association. Heart failure? None. Mortality? None. Until, of course, LDL levels are extraordinarily high, over 200—i.e. grossly abnormal. This is far beyond thresholds targeted by modern guidelines.
Above is a figure from a 2021 study of LDL cholesterol in US adults, plotted against deaths. Note that the horizontal black line on the vertical y-axis is expected death rate. The solid red line is actual death rate. Until 200 mg/dL the red line does not begin to separate from expected mortality. This, by the way, is LDL alone, not total cholesterol. Meanwhile, the AHA hits the panic button at 160 or above, labeling this its very highest risk category—well before LDL is even a risk factor for death.
All of this helps explain why lowering LDL in primary prevention has produced, if anything, hilariously small ‘benefits’. Reductions in stroke are at best fatuous. There is no effect on mortality. And even nonfatal heart attack, the prize pig of the fair, is barely touched. (Stay tuned next week, for more on this one).
Contrast this with smoking or blood pressure. When smoking or blood pressure is reduced, there are clear reductions in stroke, MI, and death. That is because the associations are, and always have been, robust and consistent. But cholesterol never had that foundation.
Which makes the current moment bizarre.
Instead of reconsidering their premise when history’s biggest and best study of risk factors showed last year that ‘high LDL’, as currently defined, has no association with heart disease or death, the AHA is doubling down.
That is because they have reversed the scientific method.
They are not starting with a strong association and asking whether modifying it helps. Instead, they are starting with an assumption—that LDL is the central cause of heart disease—then searching for data to make the assumption look true.
This is why the gargantuan efforts and enormous costs that have been poured into obsessing over, and diligently lowering, cholesterol to prevent heart disease have yielded nothing.
I once diagnosed a man with appendicitis before I knew whether he had an appendix. Bad call.
First things first: Association is the first principle in establishing a risk factor. Everything else follows.
Cholesterol doesn’t have it.
Next week I’ll write about heart attacks, specifically nonfatal ones. You’ll see why.