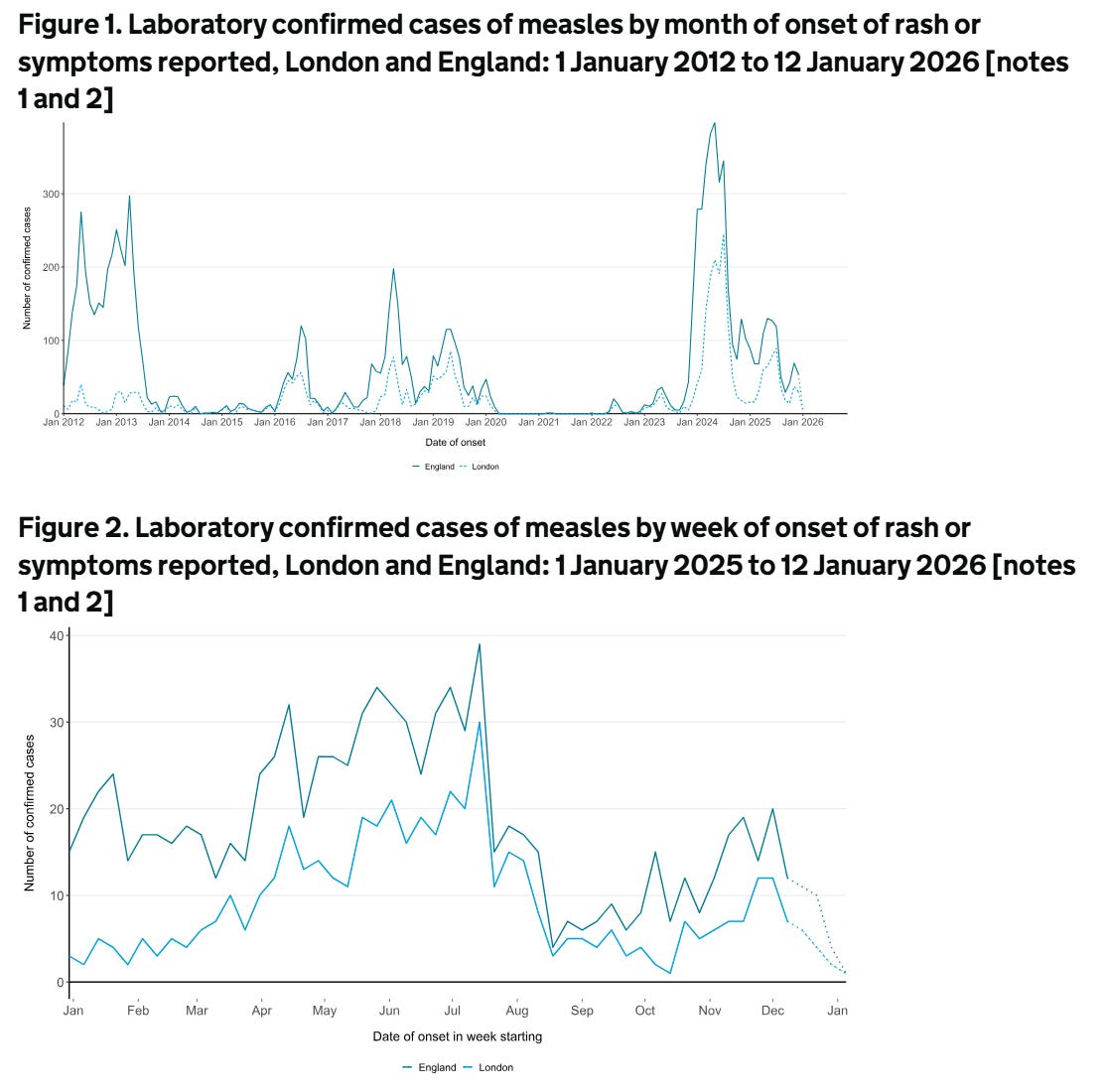
If you have multiple sclerosis (MS) and are on chronic immunosuppression, you need to check your medical records to make sure you have had the measles vaccine as a child. Due to vaccine hesitancy, MMR (measles, mumps, and rubella) vaccine uptake has dropped considerably since the late 90’s and noughties. As a result, many countries now have both endemic and epidemic levels of measles infections. This is clearly very worrying. The bad news is that the World Health Organisation (WHO) has stated that the UK is no longer considered to have eliminated measles. The WHO has said measles transmission was re-established in the UK in 2024, following a plateau in vaccination coverage and a surge in cases. A total of 3681 measles cases were recorded in England in 2024. This will underestimate the true incidence of measles, as these figures rely on accurate diagnoses and on cases being reported to the Health Security Agency.
Now, let's say you are a person with MS who did not have the MMR vaccine because your parents were worried about the safety of the MMR vaccine. You would now be vulnerable to getting infected as an adult. In the past, you could have relied on herd immunity, i.e. all the people around you who had the vaccine and are immune to measles would prevent the virus from spreading in the community and protect you. Unfortunately, herd immunity is simply not good enough. The latest figures from the UK’s Health Security Agency for England show that in 2024-2025, 91.9% of five-year-olds had received one dose of the MMR vaccine, which is largely unchanged from 2023-2024 and the lowest level since 2010-2011. Just 83.7% of 5-year-olds had received both MMR doses, down year-on-year from 83.9% and the lowest level since 2009-2010. The WHO recommends that at least 95% of children receive each vaccine to achieve herd immunity.
My worry is that people with MS will get measles, and because they are on an immunosuppressive therapy, will get complications, in particular encephalitis.
Measles encephalitis
Measles encephalitis is a serious complication of the measles virus infection that often leads to permanent brain damage or death. While measles is often thought of as a respiratory illness with a rash, the virus can infect the central nervous system. This complication occurs in approximately 1 in every 1,000 people who get measles, but it is much more common in people who are immunocompromised.
Acute measles encephalitis usually occurs during or shortly after the initial infection (often whilst the rash is still present). It is often caused by the immune system attacking the brain (an autoimmune reaction) rather than the virus directly attacking brain tissue, though direct viral invasion also happens. It is associated with a high fever, headache, stiff neck, vomiting, drowsiness, seizures, and coma. It typically begins about 6 days after the rash onset. The mortality rate is approximately 10–15%. Among survivors, about 25% suffer permanent neurological damage, such as intellectual disability, seizures, or deafness.
Subacute Sclerosing Panencephalitis (SSPE) is a rare, chronic, and fatal form of measles encephalitis. It is caused by a persistent measles virus infection in the brain that reactivates years later. It typically develops 7 to 10 years after the person has recovered from the initial measles infection. It starts with subtle behavioural changes and memory loss, progressing to muscle spasms (myoclonus), seizures, and eventually a vegetative state. It occurs in roughly 1 in 10,000 to 1 in 100,000 people who had measles, but the risk is higher for those infected with measles before the age of two.
Measles inclusion body encephalitis (MIBE) is a specific form found in people with compromised immune systems (e.g., those with HIV, organ transplants or on immunosuppressive treatments). It usually occurs a few months after the initial measles infection. It is usually fatal, with death often occurring within weeks of symptom onset.
There is no specific antiviral treatment for these forms of measles encephalitis once they have begun; healthcare professionals can only provide supportive care (hydration, seizure management, etc.) to help the body fight the infection. Therefore, the only effective protection is prevention via the MMR vaccine. The vaccine prevents the initial measles infection, thereby eliminating the risk of these neurological complications.
It is only a matter of time before a person with MS who has not received the MMR vaccine gets measles and one of the forms of measles encephalitis. I am particularly concerned about pwMS on natalizumab who will get a subacute infectious syndrome that may mimic PML or a prion disease such as Creutzfeldt-Jakob disease. PwMS on anti-CD20 therapies and S1P modulators are also at risk. PwMS treated with immune reconstitution therapies and have reconstituted their immune systems should be okay, as they can mount an immune response to the virus.
Measles hyperimmune immunoglobulin (or human normal immunoglobulin - HNIG) is used as post-exposure prophylaxis (PEP) for susceptible individuals at high risk of severe complications from measles. It provides immediate, temporary antibodies and is recommended when the MMR vaccine cannot be used or when exposure has occurred in highly vulnerable people. The eligible groups for immunoglobulin (HNIG/IVIG) are individuals who have had significant exposure to a confirmed case of measles, are not immune (no history of 2 doses of vaccine or measles disease), and are within the 6-day exposure window. This includes infants under 1 year of age, pregnant women and immunocompromised individuals (e.g., bone marrow transplant recipients, HIV/AIDS patients, those on high-dose immunosuppressive therapy). IVIG is usually recommended for immunosuppressed individuals, while intramuscular HNIG is used for pregnant women and infants. For maximum effectiveness, immunoglobulin should be administered as soon as possible after exposure, ideally within 72 hours, but it can be given up to 6 days after exposure. It is typically administered via intramuscular injection or intravenously.
HNIG/IVIG is not a replacement for vaccination. Individuals who receive HNIG/IVIG must still receive the MMR vaccine once they are no longer immunocompromised, ideally at least 6–8 months after the immunoglobulin injection. The latter is to wait for the anti-measles IgG from HNIG/IVIG to be cleared from the body, so it won’t neutralise the vaccine.
Please note that, on the NHS, approval for measles immunoglobulin treatment is generally provided by a consultant in health protection or a virologist, not by a neurologist. The latter can delay things. I speak from personal experience as I have had one patient on anti-CD20 therapy who has a large family, and none of his children have had the MMR vaccine. The reasons for not vaccinating his children are complex and related to religion and vaccine scepticism. However, when one of his children developed measles, we had to activate this pathway. Thankfully, urgent MMR serology showed he must have had the vaccine as a child. He was not born in the UK and had no documentation of his vaccine status.
Please note that it is now part of our standard practice to check all patients’ MMR status before starting chronic immunosuppressive therapy. Since starting this practice, we have identified a small number of people who have been MMR negative who have then had to have the MMR vaccine prior to initiating treatment. The problem is that once you are on an immunosuppressive therapy, you can’t have the vaccine, as it is a live vaccine. This is one of the arguments in favour of IRTs (immune reconstitution therapies) for treating MS. Once your immune system has reconstituted after cladribine, alemtuzumab or AHSCT, live vaccines are relatively safe and not contraindicated.
Do you know your MMR status? If not, you may want to know particularly if you are about to start an immunosuppressive therapy. At the same time, please be vigilant for measles in your area, and if you come into contact with someone with measles, let your HCP know.
Have any of you not had the MMR vaccine? Have you recently come into contact with someone with measles?
Accidental readers
If you have been forwarded this email and are not an MS-Selfie subscriber, please consider subscribing and helping MS-Selfie expand its resources for the broader MS community. MS-Selfie relies on subscriptions to fund its curated MS-Selfie microsite, MS-Selfie books, MS-Selfie Infocards, and other activities that extend beyond the MS-Selfie Substack newsletters.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite and other related activities, as I don’t have time to do this myself. You must be a paying subscriber to ask questions unrelated to the newsletters or podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Questions
If you have questions unrelated to the newsletters or podcasts, please email them to ms-selfie@giovannoni.net. Prof. G will try to answer them as quickly as possible.
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have any problems, please tell your healthcare professional, who can help you.