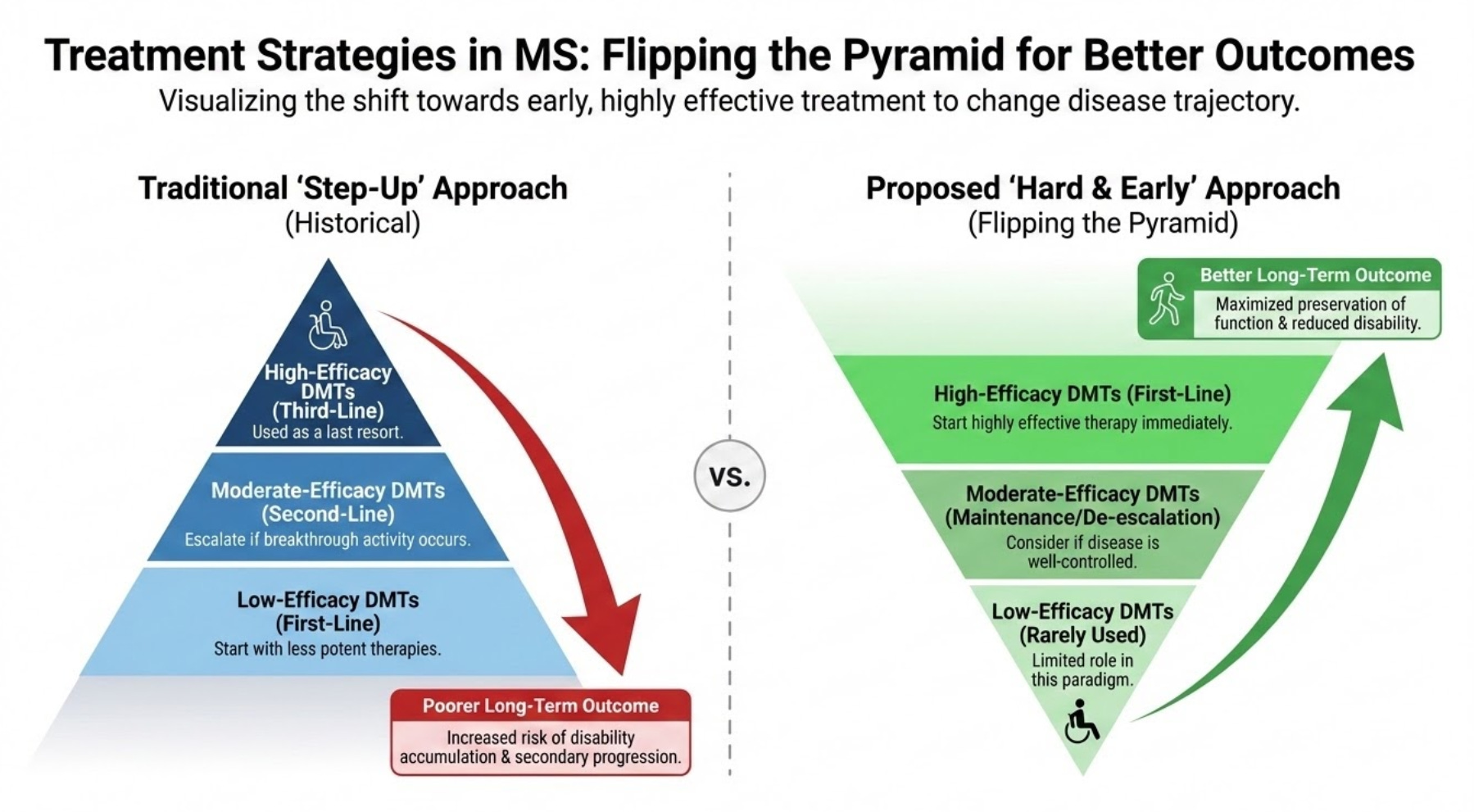
This Swedish study below explains why I keep repeating myself, i.e. ‘flip the pyramid’ and ‘smouldering MS is the real MS’.
The Swedes have investigated how different intensities of initial MS treatments impact long-term physical disability. They compared high-efficacy therapies with standard platform treatments in over 2,500 pwMS to distinguish worsening caused by relapses (relapse-associated worsening, or RAW) from progression that occurs independently of relapses (PIRA). They show that high-efficacy drugs significantly reduced the risk of relapse-associated worsening (RAW) and delayed reaching major disability milestones. However, neither treatment type showed a superior advantage in slowing progression independent of relapse activity (PIRA). This suggests that RAW and PIRA likely stem from different biological processes.
These findings indicate that while modern DMTs excel at controlling inflammation (NEIDA), additional neuroprotective strategies are necessary to halt the disease’s gradual decline associated with SAW. The results of this study advocate for aggressive early intervention (hit-hard-and-early) and the development of therapies that target smouldering processes within the CNS and repair mechanisms.
The findings of this study are not new and are in keeping with other published data. Sadly, however, there are likely too few patients treated with alemtuzumab and cladribine in this cohort and none treated with AHSCT. It is well known that the majority of pwMS on high efficacy treatments in Sweden are on off-label rituximab. I am told that Swedish neurologists now rarely use alemtuzumab, and the uptake of cladribine has also been slow. It would, however, be interesting to see if IRTs (immune reconstitution therapies), in particular alemtuzumab and AHSCT, made a difference in SAW. I say this because alemtuzumab and AHSCT are the most effective treatments we have for MS and have a profound impact on the end-organ in terms of reducing the rate of brain volume loss or brain atrophy. These two treatments do impact SAW, provided they are used early.
It is becoming increasingly difficult to justify a low-efficacy platform DMTs approach when it is clear that pwMS treated with high-efficacy therapies first-line do so much better. Do you agree?
A more interesting question for the next generation of neurologists to answer will be whether an induction-maintenance approach is superior to continued long-term immunosuppression, such as long-term anti-CD20 therapy. I note the Swedes are starting to test rituximab induction followed by cladribine as an exit strategy.
I have been advocating this approach for several years, as it reduces the risks associated with long-term immunosuppression, allows you to recover your naive B-cell population for vaccinations, and, as cladribine is CNS-penetrant, targets CNS-resident B-cells and plasmablasts that are responsible for at least one component of smouldering MS. I have little doubt that this trial will work. Sadly, it is underpowered for efficacy, but who knows if the majority of subjects go into long-term remission, it may affect how both rituximab and cladribine are used in Sweden.
If you are on long-term anti-CD20 therapy, would you consider switching to cladribine? Would you participate in a trial to test the safety and efficacy of anti-CD20 induction followed by an exit via cladribine?
Background: Several observational studies have compared high-efficacy and platform disease-modifying therapies (DMTs) with respect to long-term disability in relapsing-onset multiple sclerosis (MS), yet it remains unclear whether observed differences reflect relapse-associated worsening (RAW), progression independent of relapse activity (PIRA), or both.
Methods: We included 2,563 DMT-naïve individuals with relapsing-onset MS enrolled in a population-based study linked to the Swedish MS registry (40 clinics, 2005-2019). The exposure was an initial DMT efficacy class (platform versus high-efficacy therapy), with platform as the reference. Cox models estimated hazard ratios (HRs) with 95% confidence intervals (CIs) for RAW, PIRA, and time to EDSS 3 and 4. EDSS trajectories were modelled using mixed-effects models. Follow-up started at DMT initiation and was censored at treatment switch, discontinuation, death, drop-out, or study end.
Results: At treatment initiation, 1,987 participants started a platform DMT and 576 a high-efficacy DMT. High-efficacy therapy was associated with a lower risk of RAW (HR 0.60, 95% CI 0.38-0.92), while the risk of PIRA did not differ between treatment groups (HR 1.05, 95% CI 0.79-1.39). Risks of reaching EDSS 3 and EDSS 4 were also lower with high-efficacy DMT (EDSS 3: HR 0.26, 95% CI 0.17-0.38; EDSS 4: HR 0.32, 95% CI 0.18-0.54). EDSS trajectories increased more steeply among participants treated with the platform, with partial convergence toward the high-efficacy group over time.
Conclusions: Our findings suggest that inflammatory and relapse-independent components of MS disability respond differently to current therapies and highlight the need for complementary neuroprotective strategies.
Accidental readers
If you have been forwarded this email and are not an MS-Selfie subscriber, please consider subscribing and helping MS-Selfie expand its resources for the broader MS community. MS-Selfie relies on subscriptions to fund its curated MS-Selfie microsite, MS-Selfie books, MS-Selfie Infocards, and other activities that extend beyond the MS-Selfie Substack newsletters.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite and other related activities, as I don’t have time to do this myself. You must be a paying subscriber to ask questions unrelated to the newsletters or podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Questions
If you have questions unrelated to the newsletters or podcasts, please email them to ms-selfie@giovannoni.net. Prof. G will try to answer them as quickly as possible.
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have any problems, please tell your healthcare professional, who can help you.