Another day another gait video. If you’re a fellow gait geek, movement detective, or Anatomy in Motion learner I hope you’ll enjoy following along with this gait analysis.
Meet Our Lovely Gait Model
This video is from Haider, a student who joined us in my Toronto Flow Motion Model course last November 2024. We filmed his video to use as a potential gait analysis to look at as a group, but in the end it didn’t make the cut (sorry, Haider). The reason we didn’t use his video in the actual class was because there was a little toooo much going on and I wanted a case study that was simple and obvious to use for learning purposes.
But now that we’re out of the classroom, no holds are barred. Let’s take break this shit down! We love your complexity, Haider.
What does a knee with a recent ACL reconstruction look like in gait?
This video is a good example for how a body may look like whilst walking with a relatively recent knee operation.
Did you notice Haider’s left knee in the video?
His knee does an interesting thing where it seems to hyper-extend while also being more valgus while entering late swing to heel strike, compared to his right,
If you are someone who’s been studying the Flow Motion Model and Gary Ward’s closed chain biomechanics for any length of time, you’ll know that knee valgus and extension should not go together. Big red flag that made me want to know more.
So I emailed Haider to ask:
Did something happen to your left knee? (because of how you don't seem to want to get your mass fully on top of it and the knee holds a more valgus state and looks to be hyperextended?)
To which he replied:
“Yes, I had ACL reconstruction with a patellar graft on my left side Jan 2024. So I was about 10 months post op at the time of the course”.
WHOAH. Here’s what we can learn about the mechanics of an ACL injury and how it is showing up in Haider’s gait:
Brief overview of knee mechanics in gait
Forgive this jargony, technical breakdown of the knee, according to Gary Ward’s closed chain biomechanics. 5 people reading this might enjoy it.
* The knee in gait is best understood by looking at the articulation between the tibia and the femur.
* Our reference point for the knee joint is the position of the tibial tuberosity relative to the femur.
* The femur and tibia bones have two planes of motion they should ideally articulate against each other in: Sagittal (flexion and extension, plus a bit of anterior/posterior glide), and transverse (internal and external rotation). We should NOT see much in the frontal plane.
* There are two specific combinations of those two planes of motion we want to see in gait, and TWO ONLY:
* Flexion + External rotation (aka valgus)
* Extension + Internal rotation
* A knee hyperextension can only happen if we have the combination of extension and external rotation. This is NOT something we want to see happening in gait (sorry, Haider, but your body is doing it).
Knee external rotation refers to the internal rotation of the femur articulating on top of the tibia plateau into a range that is beyond how far the tibia internally rotates, leaving the tibia in an external rotation relative to the femur, and the knee joint itself thus in an external rotation. This happens with a knee that is bending on top of a pronating foot.
Knee internal rotation refers to the external rotation of the femur into articulating on top of the tibia plateau into a range that is beyond how far the tibia externally rotates, leaving the tibia in an internal rotation relative to the femur, and the knee joint itself thus in an internal rotation. This happens with a knee that is extending on top of a supinating foot.
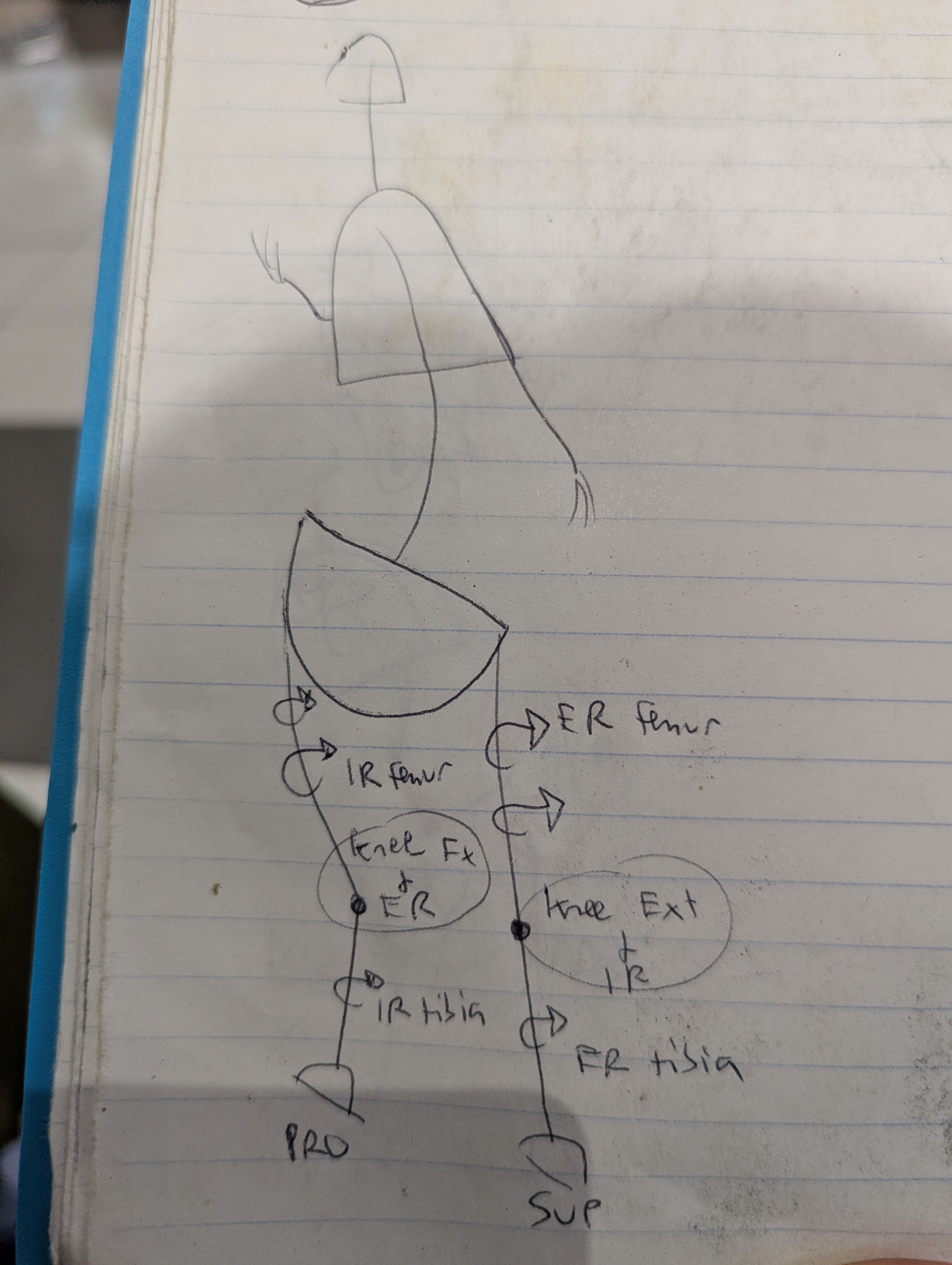
Check out my very technical drawing:
Notice that the femur and tibia both rotate the same direction, but the range of the femur is greater than the tibia, which is what gives us the rotation at the knee joint. If both bones were to simply rotate the same amount, locked together as if they were one long leg bone, then there would be no rotation at the knee joint.
External rotation and flexion of the knee happens with a femur internally rotating and a pronating foot.
Internal rotation and extension of the knee happens with a femur externally rotating and a supinating foot.
I’m repeating myself so many times because this is the MOST common sticking point people have by far in the AiM course work. It took me a few years to really wrap my head about it. But I’m slow… Anyway. Back to Haider.
Haider’s Red Flag
In Haider’s case, the red flag was his left knee extending with a femur internally rotating, giving us a knee external rotation at a moment in time when we want it to be a nice rigid extended and internally rotated knee, not a squishy hyperextended knee going into a valgus position in the air (and then landing like that, too).
A valgus position of the knee will almost always indicate an internally rotated femur, and a femur that is internally rotated will almost always tell us there is an external rotation at the knee UNLESS the foot and tibia are internally rotated MORE than the femur.
But I digress. You may now be asking the all important question…
What to do with a hyperextending knee?
Give it back the mechanics it needs in the correct combinations as per closed chain biomechanics.
Haider’s knee is missing:
Flexion + external rotation (but is already externally rotated)
Extension + internal rotation (but is already extended)
So we want to give him back these two movements but managing the excessive motions where necessary.
Its a pretty common scenario to need to block how far someone is extending their knee and encourage more external rotation at the femur while avoiding hyperextension.
If you want to follow along with me for an hour of knee exploration, perhaps you would enjoy this Movement Deep Dive I filmed back in 2021. Ahh the good ol’ COVID online teaching days. Enjoy this guided movement practice focusing on conceptualizing and experiencing the movement of the knee.
But anyway, that was a big knee tangent. Let’s get back to a few of Haider’s other biomechanical foibles, shall we?
What about that right ankle, Haider?
Something subtle that stood out in Haider’s mid-stance phase was an early heel lift on the right that I didn’t see on the left. So I asked:
Did anything happen to your right ankle? Your TCJ seems to be missing dorsiflexion compared to your left...
To which Haider Replied:
“I’ve had multiple ankle sprains on both sides but my most recent (~5 years ago) was on my right. You’re right, my right ankle DF is less than my left”
And what about your right hip?
All throughout Haider’s gait he stays in a right pelvis hike and his mass never seems to get fully off of his right leg, so I was curious and asked:
Do you have any issues with your right hip or lower back? (because of how it seems like your pelvis stays hiked on the right and your mass doesn't shift to the left to ABduct your right hip... Groin or hip flexor grumpiness at all?)
And Haider replied:
“My right hip is generally bit stiffer into external rotation and abduction. So I do have more adductor resistance to stretch on the right”.
Interesting stuff.
Final remarks
As you can see, there are a few things going on. Where would we start?
It isn’t necessarily as simple as saying “encourage pronation mechanics on his left and supination on his right”, because each leg is a little mixed up with elements of both.
For example, his right leg needs:
PRONATION MECHANICS:
* TCJ dorsiflexion (that early heel lift…)
SUPINATION MECHANICS:
* Hip extension, abduction, external rotation
* Pelvis drop
And his left leg needs:
PRONATION MECHANICS:
* Knee flexion
* Pelvis hike
* Hip adduction
SUPINATION MECHANICS:
* Knee internal rotation
* Femur external rotation
Nothing really wraps up neatly into one phase, so with Haider it might be an approach of tackling the local mechanics and then building them out holistically to combine with more joints into the phases over time.
I personally would start with the thing that stands out the most to me, which is his discombobulated knee. Start with the thing that looks the most blaringly obvious, reassess, and follow the next best bread-crumb.
Anyway, hope you found this gait analysis at least a little bit interesting and useful.
My hopes is that these analysis videos help students studying the Flow Motion Model and Anatomy in Motion to apply the mechanics to their work with clients, and perhaps even help those who want to go on to do the accredited practitioner exam (part of which includes doing a gait analysis).
If you have any questions or commentary, or would like to submit your own gait video for scrutiny, feel free to drop me a line.
Want to learn AiM in the classroom
Nothing beats mental masturbation as a learning method than actually getting into a live classroom and putting this work into your body experientially, and practicing using the assessments on others.
For those wishing to study in-person, I will be teaching the AiM Closed Chain Biomechanics course this June 6-8 2025 in Toronto. GO HERE for more info and to register, if you dig it :)